Osteoporosis ? The disease that does not receive the necessary attention
Osteoporosis is one of those diseases that affects millions of people around the world, but to which no one pays the attention it deserves. It’s like she’s invisible. It is really unfortunate how disastrous it can be for people’s lives, but at the same time it is something that can be avoided if measures are taken in time.
Table of Contents
What is osteoporosis?
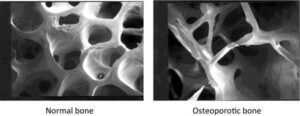
Osteoporosis is a systemic bone disease. It is characterized by reduced bone mass and altered bone microarchitecture, leading to reduced bone strength and increased risk of fractures.
It is a disease of bone metabolism that threatens both women and men. Osteoporosis is an extremely serious health problem because it is associated with increased levels of morbidity and mortality among people and attempts to treat it around the world cost insanely large funds. Epidemiological data show that in industrialized countries, between 9 and 38% of women and between 1 and 8% of men over the age of 50 suffer from osteoporosis.
How does osteoporosis occur?
Our bones, like our heart or muscles, are a specific type of tissue. As long as we are alive, every tissue in the human body is in a constant cycle of processes of decay and construction. Once fully formed, bones undergo two very important processes – modeling and remodeling.
In modeling, only one of the following two things happens within a given surface:
-
bone formation;
-
bone resorption.
The formation of bone tissue is also called ossification or osteogenesis. In this process, cells called osteoblasts lay a new layer of material to build bone. In contrast to formation, bone resorption is a process in which cells called osteoclasts destroy bone tissue, thus releasing the minerals present in the tissue into the blood.
Remodeling, in turn, is a process involving the same processes of formation and resorption, but it does not just happen one or the other, but happens together, sequentially within a given surface.
These processes are usually in different proportions depending mainly on our age. In the early years, somewhere up to about 18-20 years of age, the processes of bone formation dominate.
After our 20th anniversary, for about 10-20 years, the formation and resorption are in approximate balance and from then on the resorption begins to take control. It is the resultant accumulation of the resorption process over time that leads to a decrease in the mass and density of the bones, which, reaching a certain level of density, is called osteoporosis.
Risk groups and factors
Unfortunately, no one is insured against osteoporosis, but some are more at risk than others. The most at risk group are menopausal women. The reason for this is mainly the fact that at the onset of menopause, the secretion of the hormone estrogen stops. Estrogen is extremely important for bone metabolism in both women and men. Hormone deficiency significantly increases the production of osteoclasts, which are the main drivers of the resorption process.
Estrogen levels are not the only factor influencing the risk of developing osteoporosis.
Other risk factors are:
- age;
- glucocorticoid therapy;
- presence of previous bone fractures;
- presence of previous fractures of the femur in the family; smoking;
- alcohol consumption; presence of certain diseases:
- Rheumatoid arthritis;
- Diabetes;
- Osteogenesis of the imperfect;
- Hyperthyroidism;
- Hypogonadism or early premenopause;
- Chronic malnutrition;
- Poor absorption of certain nutrients;
- Chronic liver and kidney diseases.
A number of scientific data suggest a possible link between the presence of metabolic syndrome and osteoporosis, but the data are still conflicting. Work is also underway to determine the relationship between genes, the immune system and the disease.
Although women are the main group of people at increased risk of osteoporosis, the disease is often very common in men. According to an NHANES report, between 3 and 6% of men suffer from osteoporosis and between 28 and 47% suffer from osteopenia (reduced bone mass prior to osteoporosis diagnosis).
The risk in men is again related to both the above risk factors and hormonal levels – in addition to the hormone estrogen and testosterone. With age, estrogen and testosterone levels in men decrease by about 1% per year. A number of scientific studies have shown that the incidence of osteoporosis in men over the age of 65 who have low testosterone levels (lower than 200 ng / dl) is twice as high as in men with normal testosterone levels. higher than 400 ng / dl) (12.3% vs. 6%). An even higher incidence of the disease was observed in men with low estrogen levels (less than 10 pg / ml) and in those with normal (higher than 20 pg / ml) – 15.4% vs. 2.8%.
Why is osteoporosis dangerous?
Due to the lower bone mass and density, the main problem in the presence of osteoporosis is the increased risk of bone fractures. Younger readers are probably wondering what can be so dangerous about a broken bone, but in order to get a good idea of the problem, we need to put ourselves in the place of an older person, over 55-60 years of age. The majority of older people are generally immobilized in general and even simple movements such as getting out of bed or walking are difficult for them.
In most adults, the risk of falling is extremely high – over 50%. In the presence of osteoporosis, any fall can lead to a serious fracture. One of the most common fractures in osteoporosis is that of the thighs and hips. With such a fracture, most older people become unable to take care of themselves and must be taken care of by another person. Fractures can be so dangerous that, according to the available hip fractures, they increase the risk of death in the next 1 year by between 8 and 36%. The presence of a fracture in the hips and thighs increases the risk of future fractures by 2.5 times.
And although falls are the main cause of more serious fractures, depending on the degree of thinning of the bones, even simple things like sneezing or involuntary collision with another person / object can lead to injuries. Osteoporosis brings with it not only a deteriorating quality of life (especially in combination with another common disease in adults – sarcopenia , but also a real danger of death.
Diagnosis
For the diagnosis of osteoporosis, bone mineral density (BMD) is most often tested. Bone X-ray absorptiometry (DXA) is mainly used to study bone density and mass, and the whole body or only certain parts of it can be examined – the femoral neck, the spine (mostly the lumbar part) or 33% of the radial bone. (forearm).
The evaluation of the analysis comes in the form of a T-score. A T-score ≤ −2.5 diagnoses osteoporosis, and a T-score between -1.0 and -2.5 diagnoses osteopenia. T-score ≥ -1.0 is considered normal bone strength and density.
It is important to note that a T-score diagnosis can only be made in men and women over the age of 50. For younger men and women, a Z-score is used. A score of Z-score <-2.0 is considered clinically significant. When using the Z-score, the diagnosis of osteoporosis or osteopenia is not very correct. A Z-score <-2.0 is interpreted as “lower than normal for the respective age”, and a Z-score> -2.0 is interpreted as “normal for the respective age”.
Science is also advancing in the study of certain biomarkers as a means of diagnosing osteoporosis and bone metabolism. Such markers are, for example, markers associated with bone formation (osteocalcin, alkaline phosphatase, procollagen type 1 carboxy-terminal propeptide and procollagen 1 amino-terminal propeptide), as well as those associated with bone resorption (tartrate-resistant acid phosphate resistant). type 1 c-terminal part). However, much work remains to be done in this direction.
Prevention and treatment
Osteoporosis is likened to being an invisible disease, mainly because symptoms only appear when things get significantly worse. The main recommendations of health organizations are to examine people over the age of 50 if they have had a fracture after reaching that age, or all people over the age of 65, whether or not they have had fractures.
Osteoporosis is a disease that can be prevented, but the recommendations for research at such a late stage in life unfortunately significantly reduces the possibility of avoiding it. No less important is the fact that most young people are not sufficiently informed.
Recommendations for the prevention of osteoporosis are also valid for its treatment.
Reduce alcohol consumption
It is recommended to limit alcohol consumption to no more than 2 units per day. 1 unit of alcohol is equal to 10 ml or 8 grams of pure alcohol. Referring to some of the more popular types of alcoholic beverages, 2 units equals about:
-
500 ml of beer;
-
150 ml of wine;
-
50 ml of hard alcohol (vodka, whiskey and others).
Reducing smoking
Smoking significantly increases the risk of osteoporosis and fractures. The risk is highest in current smokers, but remains elevated even in people who have stopped smoking.
Get enough vitamin D and calcium
Although many substances are associated with bone metabolism, vitamin D and calcium deserve special attention.
99% of the calcium in our body is found in the bones, but the mineral also plays key roles in the metabolism of most cells. When we do not get enough through food, our body is forced to increase the levels of resorption in the bones to get the mineral. The recommended amount of calcium is in the range of 1000 mg / day for both men and women. For people over 70 years of age, the recommendations are slightly higher – 1200 mg / day. It is not recommended to systematically take larger amounts than 1500 mg, as on the one hand they do not bring additional benefits, and on the other hand the long-term safety of higher doses is not completely clear.
Vitamin D is also critical for maintaining healthy bones, with current recommendations in the range of 800-1000 IU / day. It is recommended to be supplied with calcium, as it is necessary for and improves intestinal calcium absorption (30) , although according to some data the improvement is minimal (. On the other hand, only the combination of vitamin D and calcium, but not both, shows a reduced risk of falling in the elderly, which is particularly important for those diagnosed with osteoporosis.
Taking other dietary supplements
Meta-analyzes show that intake of fish oil / omega-3 and soy isoflavones may be beneficial.
Sources used :
- Cosman F, de Beur SJ, LeBoff MS, Lewiecki EM, Tanner B, Randall S, et al. Clinician’s Guide to Prevention and Treatment of Osteoporosis. Osteoporos Int. 2014 Oct;25(10):2359–81.
- Faibish D, Ott SM, Boskey AL. Mineral changes in osteoporosis: a review. Clin Orthop Relat Res. 2006 Feb;443:28–38.
- Pietschmann P, Rauner M, Sipos W, Kerschan-Schindl K. Osteoporosis: An Age-Related and Gender-Specific Disease – A Mini-Review. Gerontology. 2009;55(1):3–12.
- Kling JM, Clarke BL, Sandhu NP. Osteoporosis prevention, screening, and treatment: a review. J Womens Health (Larchmt). 2014 Jul;23(7):563–72.
- Wade SW, Strader C, Fitzpatrick LA, Anthony MS, O’Malley CD. Estimating prevalence of osteoporosis: examples from industrialized countries. Arch Osteoporos. 2014 Dec 16;9(1):182.
- Seeman E. Invited Review: Pathogenesis of osteoporosis. J Appl Physiol. 2003 Nov;95(5):2142–51.
- Bone Modeling and Remodeling. Basic Appl Bone Biol. 2014 Jan 1;75–90.
- Bijelic R, Milicevic S, Balaban J. Risk Factors for Osteoporosis in Postmenopausal Women. Med Arch (Sarajevo, Bosnia Herzegovina). 2017 Feb;71(1):25–8.
- Cohen A. PREMENOPAUSAL OSTEOPOROSIS. Endocrinol Metab Clin North Am. 2017;46(1):117.
- Wong SK, Chin K-Y, Suhaimi FH, Ahmad F, Ima-Nirwana S. The Relationship between Metabolic Syndrome and Osteoporosis: A Review. Nutrients. 2016 Jun 7;8(6).
- Rocha-Braz MGM, Ferraz-de-Souza B. Genetics of osteoporosis: searching for candidate genes for bone fragility. Arch Endocrinol Metab. 2016 Aug;60(4):391–401.
- Pietschmann P, Mechtcheriakova D, Meshcheryakova A, Föger-Samwald U, Ellinger I. Immunology of Osteoporosis: A Mini-Review. Gerontology. 2016;62(2):128–37.
- Stathopoulos I, Ballas E, Lampropoulou-Adamidou K, Trovas G. A review on osteoporosis in men. Hormones. 2014 Dec 9;
- Abrahamsen B, van Staa T, Ariely R, Olson M, Cooper C. Excess mortality following hip fracture: a systematic epidemiological review. Osteoporos Int. 2009 Oct 7;20(10):1633–50.
- Colоn-Emeric C, Kuchibhatla M, Pieper C, Hawkes W, Fredman L, Magaziner J, et al. The contribution of hip fracture to risk of subsequent fractures: data from two longitudinal studies. Osteoporos Int. 2003 Nov 1;14(11):879–83.
- Reginster J-Y, Beaudart C, Buckinx F, Bruyère O. Osteoporosis and sarcopenia: two diseases or one? Curr Opin Clin Nutr Metab Care. 2016 Jan;19(1):31–6.
- Kerr C, Bottomley C, Shingler S, Giangregorio L, de Freitas HM, Patel C, et al. The importance of physical function to people with osteoporosis. Osteoporos Int. 2017 May 6;28(5):1597–607.
- Li G, Thabane L, Papaioannou A, Ioannidis G, Levine MAH, Adachi JD. An overview of osteoporosis and frailty in the elderly. BMC Musculoskelet Disord. 2017;18(1):46.
- Burch J, Rice S, Yang H, Neilson A, Stirk L, Francis R, et al. Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment: the secondary prevention of fractures, and primary prevention of fractures in high-risk groups. Health Technol Assess. 2014 Feb;18(11):1–180.
- Chan CY, Mohamed N, Ima-Nirwana S, Chin K-Y. A Review of Knowledge, Belief and Practice Regarding Osteoporosis among Adolescents and Young Adults. Int J Environ Res Public Health. 2018;15(8).
- Barker KL, Toye F, Lowe CJM. A qualitative systematic review of patients’ experience of osteoporosis using meta-ethnography. Arch Osteoporos. 2016;11(1):33.
- Weaver CM, Gordon CM, Janz KF, Kalkwarf HJ, Lappe JM, Lewis R, et al. The National Osteoporosis Foundation’s position statement on peak bone mass development and lifestyle factors: a systematic review and implementation recommendations. Osteoporos Int. 2016 Apr;27(4):1281–386.
- Curtis EM, Moon RJ, Dennison EM, Harvey NC, Cooper C. Recent advances in the pathogenesis and treatment of osteoporosis. Clin Med. 2015 Dec;15 Suppl 6(Suppl 6):s92-6.
- Compston J, Cooper A, Cooper C, Gittoes N, Gregson C, Harvey N, et al. UK clinical guideline for the prevention and treatment of osteoporosis. Arch Osteoporos. 2017 Dec;12(1):43.
- Øyen J, Gram Gjesdal C, Nygård OK, Lie SA, Meyer HE, Apalset EM, et al. Smoking and body fat mass in relation to bone mineral density and hip fracture: the Hordaland Health Study. PLoS One. 2014;9(3):e92882.
- Kanis JA, Johnell O, Oden A, Johansson H, De Laet C, Eisman JA, et al. Smoking and fracture risk: a meta-analysis. Osteoporos Int. 2005 Feb 3;16(2):155–62.
- Weaver CM, Alexander DD, Boushey CJ, Dawson-Hughes B, Lappe JM, LeBoff MS, et al. Calcium plus vitamin D supplementation and risk of fractures: an updated meta-analysis from the National Osteoporosis Foundation. Osteoporos Int. 2016 Jan;27(1):367–76.
- Candelas G, Martinez-Lopez JA, Rosario MP, Carmona L, Loza E. Calcium supplementation and kidney stone risk in osteoporosis: a systematic literature review. Clin Exp Rheumatol. 30(6):954–61.
- Li K, Wang X-F, Li D-Y, Chen Y-C, Zhao L-J, Liu X-G, et al. The good, the bad, and the ugly of calcium supplementation: a review of calcium intake on human health. Clin Interv Aging. 2018;13:2443–52.
- Christakos S, Dhawan P, Porta A, Mady LJ, Seth T. Vitamin D and intestinal calcium absorption. Mol Cell Endocrinol. 2011 Dec 5;347(1–2):25–9.
- Gallagher JC, Yalamanchili V, Smith LM. The effect of vitamin D on calcium absorption in older women. J Clin Endocrinol Metab. 2012 Oct;97(10):3550–6.
- Wu H, Pang Q. The effect of vitamin D and calcium supplementation on falls in older adults. Orthopade. 2017 Sep 17;46(9):729–36.
- Orchard TS, Pan X, Cheek F, Ing SW, Jackson RD. A systematic review of omega-3 fatty acids and osteoporosis. Br J Nutr. 2012 Jun;107 Suppl 2(0 2):S253-60.
- Wei P, Liu M, Chen Y, Chen D-C. Systematic review of soy isoflavone supplements on osteoporosis in women. Asian Pac J Trop Med. 2012 Mar 1;5(3):243–8.
- Ireland A, J Rittweger J. Exercise for osteoporosis: how to navigate between overeagerness and defeatism. J Musculoskelet Neuronal Interact. 2017;17(3):155–61.
People also look for :
-
Asthma and Sports ? Is the Combination Possible ?
-
Corn – Health Benefits – Negatives everything you have to know before eating
-
Mineral deficiency and mineral toxicity
-
Ginger – Better in a food Supplement than in Spice for Cooking